Nonlinear PK, TMDD, and PBPK
Understand when standard PK breaks down and how TMDD and PBPK provide more mechanistic representations.
Tip
What you’ll build today: intuition for when linear PK assumptions fail and how TMDD and PBPK extend modeling toward mechanism and physiology.
Learning Objectives
By the end of this lesson, you will be able to:
- Recognize nonlinear PK behavior
- Understand the idea behind target-mediated drug disposition (TMDD)
- Understand what PBPK models represent
- Know when these approaches are useful
Key Ideas
So far, most PK thinking assumed:
- linear kinetics
- proportionality (dose ↑ → exposure ↑ proportionally)
But in many real systems:
PK can be nonlinear
This happens when processes become:
- saturable
- capacity-limited
- target-driven
Why This Lesson Matters
Standard compartment models work well for many drugs.
But they can fail when:
- binding targets affect PK
- transporters saturate
- physiology matters
This is where more mechanistic approaches come in.
Nonlinear PK
Nonlinear PK occurs when:
- clearance changes with concentration
- exposure is not proportional to dose
Example:
- doubling dose → more than double AUC
Sources of Complexity Beyond Standard PK
When standard PK assumptions fail, the reasons may differ.
Broadly:
- nonlinear processes → saturation, capacity limits
- target-mediated processes → drug–target interactions
- physiological complexity → organ-level representation
These lead to different modeling approaches.
TMDD and PBPK solve different problems.
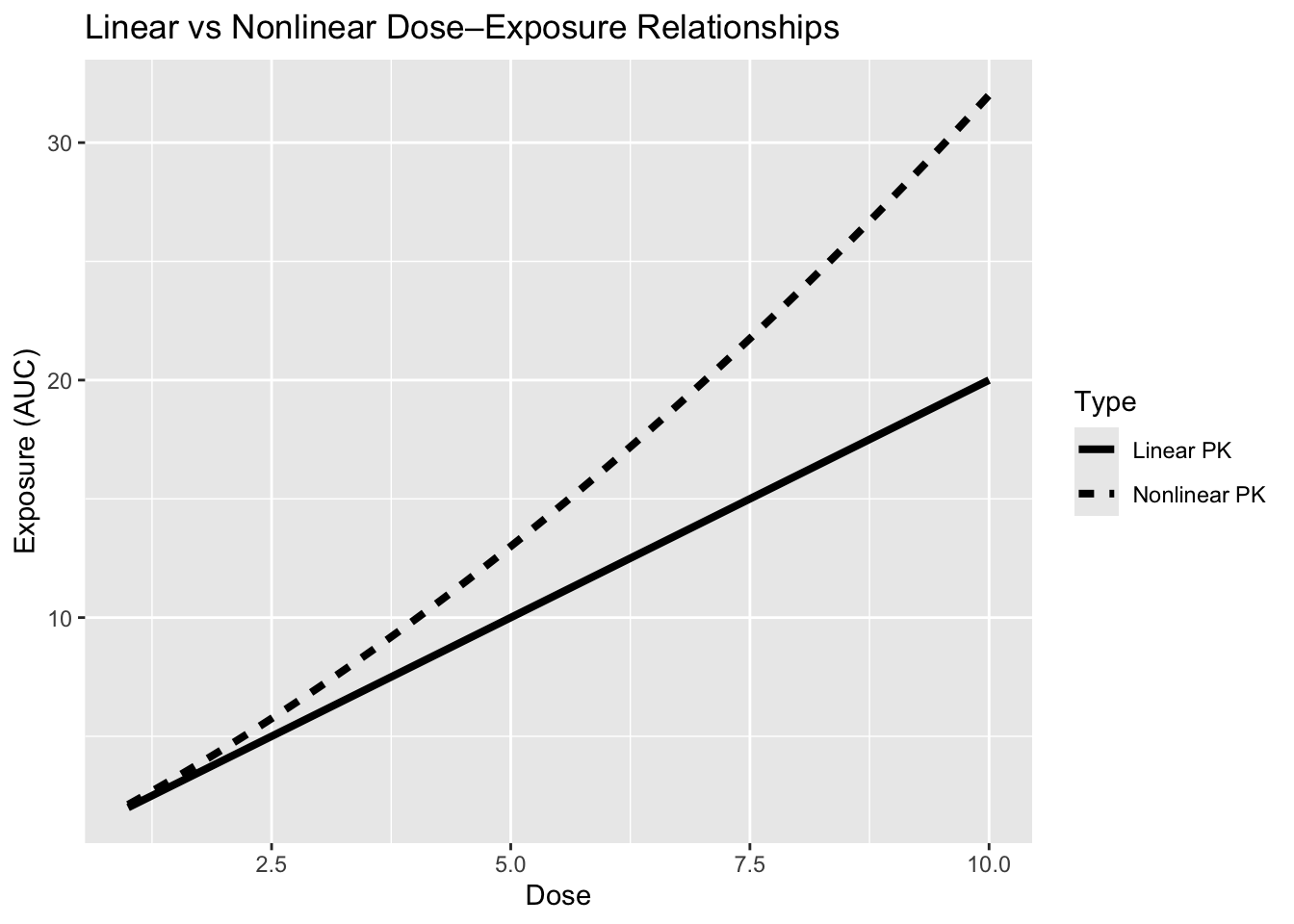
Worked Example: Linear vs Nonlinear PK
Interpretation:
- linear → proportional exposure increase
- nonlinear → exposure changes disproportionately with dose
TMDD (Target-Mediated Drug Disposition)
TMDD occurs when drug–target interaction meaningfully alters pharmacokinetics.
Common in:
- monoclonal antibodies
- biologics
Key idea:
- target binding affects clearance
TMDD extends standard PK by allowing the biological target itself to influence drug disposition.

Figure. Conceptual structure of a TMDD model.
Free drug (\(L\)) binds to a biological target or receptor (\(R\)), forming a drug–target complex (\(RL\)). Association (\(k_{on}\)) and dissociation (\(k_{off}\)) govern binding, while complex removal can contribute to drug elimination.
Unlike standard PK:
Drug → eliminationTMDD introduces:
Drug → target binding → complex → eliminationThis creates concentration-dependent clearance behavior.
Characteristic TMDD Behavior
Because target binding can become saturated, clearance may change across concentrations.

Figure. Conceptual concentration–time profile in TMDD.
At high concentrations, target pathways may become saturated and PK can appear approximately linear. As concentrations decrease, target-mediated processes become increasingly important, creating changing slopes and nonlinear behavior.
Typical phases:
- A: rapid initial decline
- B: target saturation → slower decline
- C: mixed behavior as saturation decreases
- D: target-mediated clearance becomes more visible
This means:
- target may become saturated
- clearance may change over time
- exposure can become nonlinear
Insight
In TMDD, the drug and target interact in a way that shapes both PK and PD.
Note
At low concentrations, binding may dominate; at high concentrations, saturation may occur.
PBPK (Physiologically-Based PK)
PBPK models represent:
the body as a system of physiological compartments
They include:
- organs (liver, kidney, etc.)
- blood flows
- tissue partitioning

Figure. Conceptual structure of a physiologically-based pharmacokinetic (PBPK) model.
Drug enters systemic circulation and distributes between organ compartments through arterial and venous blood flow. Each compartment represents a physiological tissue or organ: LU = lung, HT = heart, BR = brain, MU = muscle, AD = adipose tissue, SK = skin, LI = liver, BO = bone, KI = kidney, PA = pancreas, SP = spleen, ST = stomach, GU = gut, and RB = remainder of body.
Drug elimination may occur through specific organs (commonly liver and kidney). CLint denotes intrinsic clearance—the inherent ability of an eliminating organ (typically liver) to remove drug independent of blood flow limitations.
PBPK models make physiological assumptions explicit.
What PBPK Adds
Compared to standard models:
- more mechanistic
- more physiologically interpretable
- more transferable across populations
- supports extrapolation across scenarios
Expanding the Idea
PBPK is useful for:
- predicting drug behavior in new populations
- extrapolating across species
- understanding physiology-driven differences
Why This Matters for Decisions
These models support:
- dose selection for biologics
- pediatric extrapolation
- drug–drug interaction prediction
Strategies
- Start with simple models
- Move to TMDD or PBPK when needed
- Use mechanistic models when extrapolation is required
Common Mistakes
- Assuming linearity always holds
- Using complex models without justification
- Ignoring biological context
Practice Problems
- What causes nonlinear PK?
- What is TMDD?
- What does PBPK represent?
TipStep-by-Step Solutions
- Saturation or capacity limits
- PK influenced by target binding
- Physiological compartments and flows
Summary
Nonlinear PK, TMDD, and PBPK:
- extend beyond simple models
- incorporate biology and physiology
- are used when standard assumptions break
TipQuick Tips
- Nonlinearity = dose ≠ proportional exposure
- TMDD = target affects PK
- PBPK = physiology-driven modeling
- Use complexity only when needed