Exposure–Response Thinking
Understand how drug exposure connects to clinical response and how this relationship drives pharmacometric decisions.
Tip
What you’ll build today: a clear mental model of how exposure links to response—and how this relationship drives dosing and clinical decisions.
Learning Objectives
By the end of this lesson, you will be able to:
- Define exposure–response relationships
- Explain why exposure is used instead of dose
- Interpret basic exposure–response patterns
- Understand how exposure–response supports decision-making
Key Ideas
In pharmacometrics, we rarely care about dose alone.
Instead, we care about:
What exposure does the patient experience, and how does that affect response?
This leads to a fundamental relationship:
- Exposure → Response
Where:
- Exposure = AUC, Cmax, concentration
- Response = efficacy, safety, biomarker, clinical outcome
The Exposure–Response Chain
Drug response is usually understood as a sequence:
Dose
↓
Exposure (PK)
↓
Response (PD)This means:
- dose determines exposure
- exposure drives response
- response determines outcomes
This framework connects:
- pharmacokinetics (PK)
- pharmacodynamics (PD)
and forms the foundation of pharmacometrics.
Why This Lesson Matters
Two patients can receive the same dose but have:
- different clearance
- different exposure
- different outcomes
So dose alone is not enough.
Exposure is the bridge between dosing and response.
Dose vs Exposure
Dose
- What we give
Exposure
- What the body experiences
Response
- What the drug does
Insight: Dose does not cause response directly—exposure does.
Warning
Assuming dose-response without considering exposure can lead to incorrect conclusions.
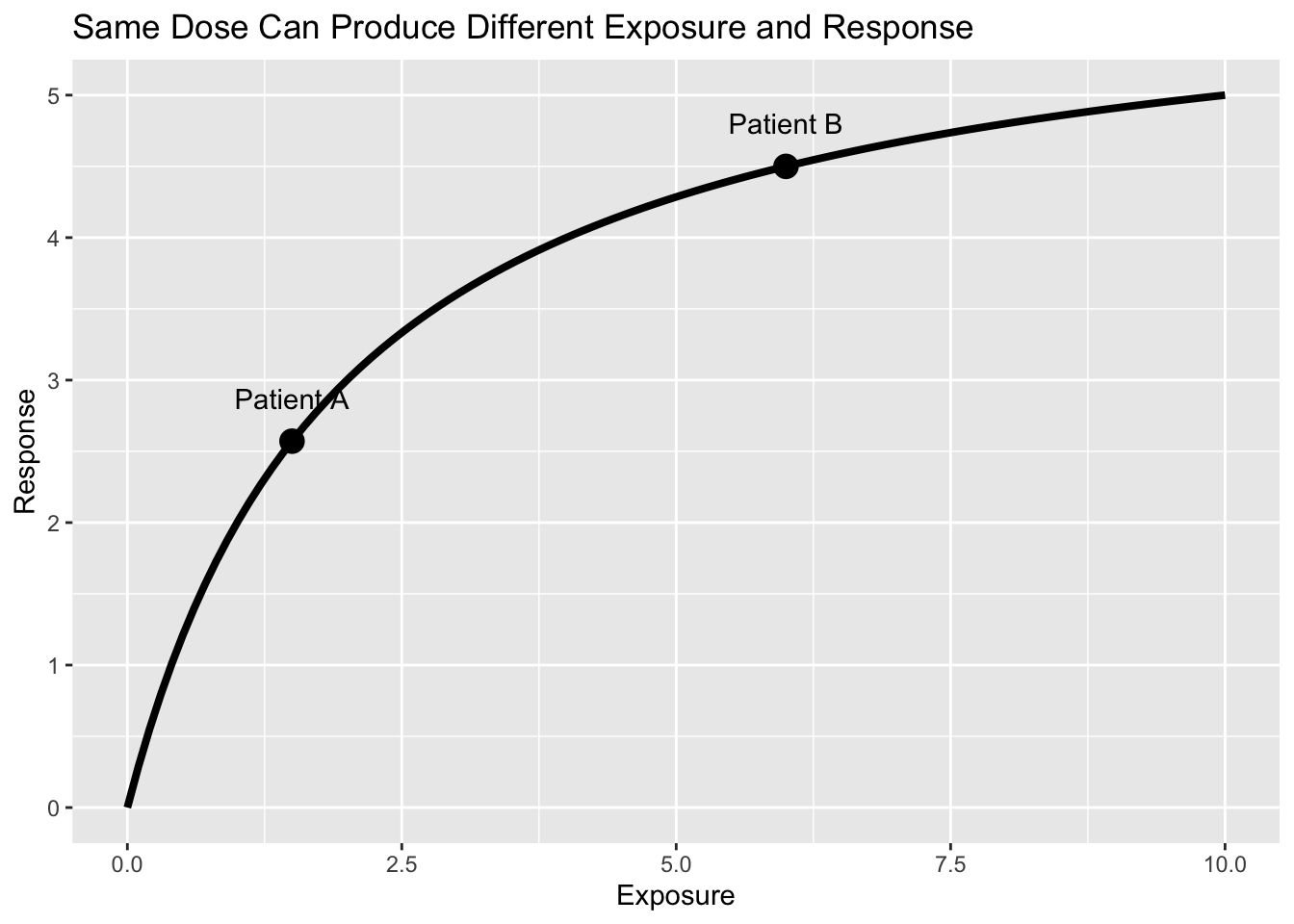
Worked Example: Same Dose, Different Outcomes
Imagine:
- Patient A → lower exposure → weaker response
- Patient B → higher exposure → stronger response
Even with the same dose:
- exposure changes
- outcomes change
Common Exposure–Response Patterns
Linear
Response increases proportionally with exposure.
Conceptually:
\[ Response \propto Exposure \]
Interpretation:
- more exposure → more response
- no plateau is reached
This relationship is simple but often unrealistic at high exposure.
Emax (Saturating)
Response increases initially but eventually approaches a maximum effect.
Conceptually:
\[ Response= \frac{ E_{max}\cdot Exposure }{ EC_{50}+Exposure } \]
Where:
- \(E_{max}\) = maximum achievable response
- \(EC_{50}\) = exposure producing 50% of maximum response
Interpretation:
- low exposure → response increases rapidly
- higher exposure → additional exposure produces smaller gains
- eventually response plateaus near maximum effect
A common extension is the sigmoid Emax (Hill) relationship, where response changes more gradually at low exposure and more sharply near the middle of the curve.
This is one of the most common exposure–response relationships in pharmacometrics.
Threshold
Little or no response occurs until exposure exceeds a minimum level.
Conceptually:
\[ Exposure < Threshold \rightarrow Response \approx 0 \]
Interpretation:
- exposure below threshold → little effect
- exposure above threshold → measurable response begins
Insight
Exposure–response relationships define both efficacy and safety boundaries.
Note
The goal is often to find an exposure range that maximizes benefit and minimizes risk.
The Goal Is Often an Exposure Range
Exposure–response is rarely about maximizing exposure.
Instead, many drugs have:
- exposure too low → insufficient efficacy
- exposure too high → toxicity
This creates:
an optimal exposure window
The goal of dosing is often to place most patients inside that range.
Why This Matters for Decisions
Exposure–response drives:
- dose selection
- dose adjustments
- safety limits
- therapeutic windows
Example:
- Too low exposure → no efficacy
- Too high exposure → toxicity
👉 The goal is to stay in the optimal exposure range
Strategies
- Analyze exposure rather than dose
- Explore both efficacy and safety endpoints
- Consider variability across patients
- Use models to predict exposure distributions
Common Mistakes
- Using dose as a proxy for exposure
- Ignoring inter-individual variability
- Overinterpreting limited data
- Assuming linear relationships
Practice Problems
- Why is exposure more important than dose?
- What is an exposure–response relationship?
- What happens at very high exposure levels?
TipStep-by-Step Solutions
- Because exposure reflects what the body actually experiences
- The relationship between drug exposure and clinical effect
- Response may plateau or toxicity may increase
Summary
Exposure–response:
- links PK to clinical outcomes
- explains variability in response
- guides dosing decisions
It is one of the most important concepts in pharmacometrics.
TipQuick Tips
- Dose → exposure → response
- Focus on exposure, not dose
- Look for nonlinear patterns
- Consider both efficacy and safety
- Use exposure to guide decisions