Bioavailability (F)
Build intuition for bioavailability and understand why administered dose is not always equal to systemic exposure.
Tip
What you’ll build today: intuition for how much drug actually reaches circulation and why dose does not automatically equal exposure.
Learning Objectives
By the end of this lesson, you will be able to:
- Define bioavailability conceptually
- Explain how bioavailability affects exposure
- Distinguish amount entering from rate of entry
- Interpret low vs high bioavailability correctly
Key Ideas
Bioavailability describes:
how much of the administered dose reaches systemic circulation
Bioavailability is often represented as:
\[ F \]
Conceptually:
\[ \text{Systemic Amount}=F\times Dose \]
where:
- larger \(F\) → more drug reaches circulation
- smaller \(F\) → less drug reaches circulation
Insight: Bioavailability determines how much gets in, not how quickly it gets in.
Warning
Low bioavailability does not necessarily mean slow absorption.
A drug may enter quickly but only a small fraction may ultimately reach circulation.
Why Bioavailability Matters
After administration:
- not all drug necessarily enters circulation
- some may not absorb
- some may be lost before reaching systemic circulation
That means:
Dose administered ≠ dose reaching circulation
This distinction is fundamental in pharmacometrics.
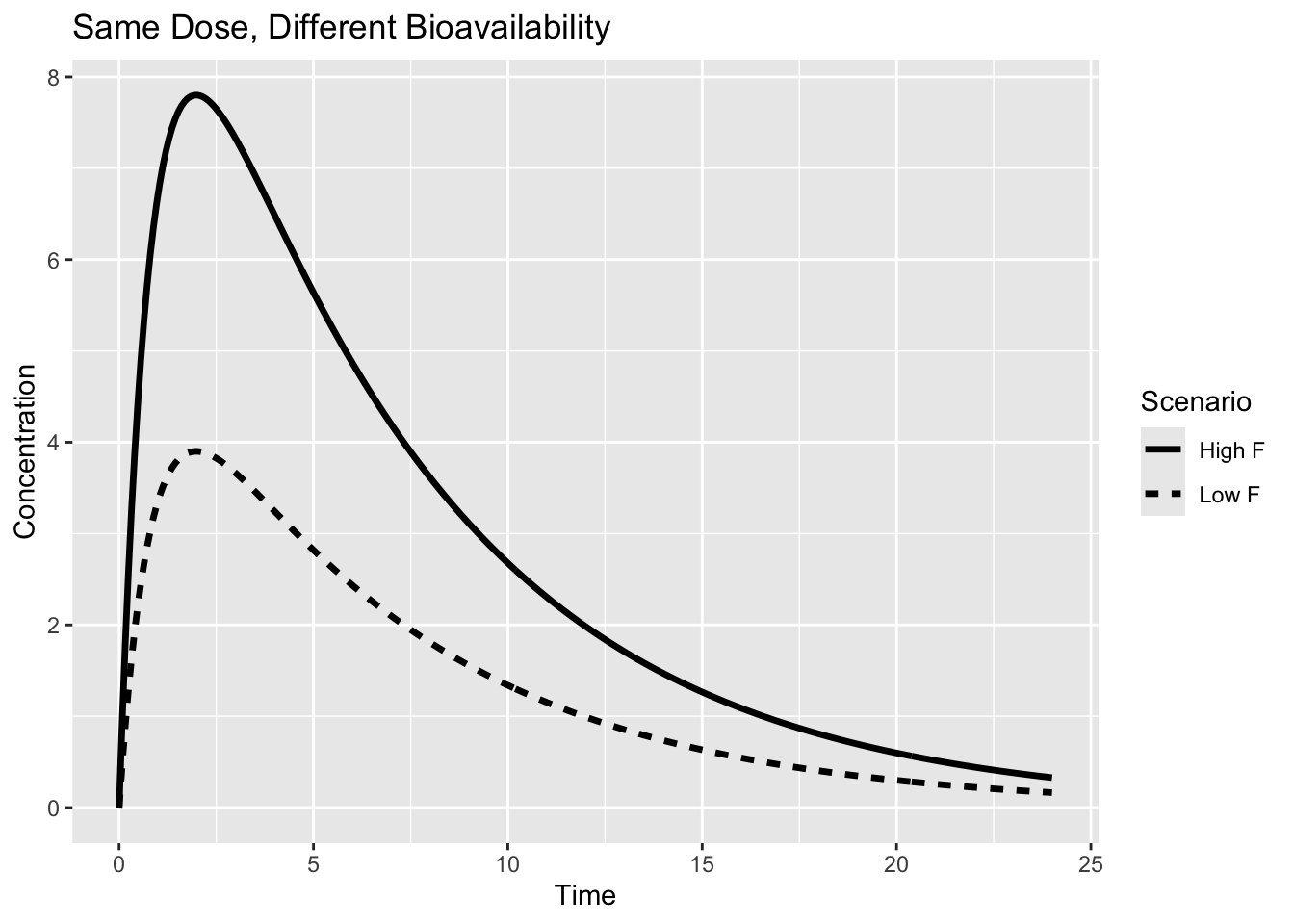
Worked Example: Same Dose, Different Bioavailability
Imagine two patients receive the same oral dose.
- Patient A → high bioavailability
- Patient B → low bioavailability
What happens?
- Patient A → greater exposure
- Patient B → lower exposure
The administered dose is identical.
But the amount entering circulation differs.
Notice:
- timing remains similar
- profile shape remains similar
- total exposure changes
Expanding the Example
Now compare another familiar scenario.
Intravenous administration:
\[ F=1 \]
Oral administration:
\[ F<1 \]
flowchart TB D[Dose] D --> A[Absorption] A --> F[Fraction reaches circulation] F --> C[Observed concentration]
Not all administered drug necessarily becomes observable in plasma.
This means:
- dose alone does not determine exposure
- bioavailability changes how much exposure is possible
Clinical Interpretation
Bioavailability helps explain:
- differences between oral and IV administration
- formulation differences
- food effects
- variability across products
- differences in exposure despite equal dose
It is especially important for:
- comparing formulations
- interpreting exposure differences
- understanding oral dosing
Insight
A useful mental model:
Absorption rate determines how quickly drug arrives.
Bioavailability determines how much drug arrives.
Note
Always ask:
“Is exposure changing because less drug entered—or because drug entered more slowly?”
Strategies
- Separate amount entering from timing of entry
- Compare exposure across routes
- Interpret low exposure cautiously
- Ask whether bioavailability or elimination explains the observation
Common Mistakes
- Assuming administered dose equals systemic exposure
- Confusing bioavailability with absorption rate
- Treating low concentration as low dose
- Ignoring route of administration
Practice Problems
- What does bioavailability represent?
- Does lower bioavailability mean slower absorption?
- Why can two patients receiving the same dose show different exposure?
TipStep-by-Step Solutions
- The fraction of administered dose reaching circulation
- No—amount and timing are different concepts
- Because different fractions of dose may reach circulation
Summary
Bioavailability determines:
- how much drug reaches circulation
- how much exposure is possible
- why dose does not equal systemic amount
Understanding bioavailability helps separate:
- administered dose
- delivered dose
- observed exposure
TipQuick Tips
- F controls amount entering
- Dose ≠ systemic amount
- Faster absorption ≠ higher F
- Exposure depends on delivered amount
- Always separate amount from timing